After reading this post you will learn the following about Dentigerous Cyst
INTRODUCTION (DEFINITION, GENERAL FEATURES, OTHER NAMES)
ETIOLOGY
CLINICAL FEATURES
RADIOGRAPHIC FEATURES
HISTOPATHOLOGIC FEATURES
TREATMENT & PROGNOIS
POTENTIAL COMPLICATIONS
INTRODUCTION
DEFINITION
"Dentigerous cyst can be defined as an odontogenic cyst that surrounds the crown of an impacted tooth; caused by fluid accumulation between the reduced enamel epithelium and the enamel surface, resulting in a cyst in which the crown is located within the lumen"
Dentigerous Cyst
is attached to the associated tooth’s neck/cementoenamel junction(CEJ)
One of the most common types of developmental odontogenic cyst, estimated to be about 20% of all jaw cysts
About 10% of impacted teeth have formed a dentigerous cyst
It usually involves crown of a normal permanent tooth
Rarely surrounds a deciduous tooth
OTHER NAME – Follicular cyst
According to Browne and Smith (1991) the term ‘dentigerous cyst’ is preferable to that of ‘follicular cyst’, as the latter implies a derivation from the tooth follicle which is a mesodermal structure. Also, the term follicular cyst is most commonly used to refer to follicular cysts of the ovary, and also to hair follicle cysts. As Browne has pointed out, the literal meaning of dentigerous is ‘tooth bearing’, and this term is most appropriate for the lesion
CLINICAL FEATURES
Associated with crown of an impacted, embedded or unerupted tooth
Sometimes involve complex compound odontoma or a supernumerary tooth
SITE – Common sites –
MANDIBULAR THIRD MOLAR
MAXILLARY CANINE
MAXILLARY THIRD MOLAR
MANDIBULAR SECOND PREMOLAR
(since these are the most commonly impacted teeth)
AGE – Most lesions present in second and third decades
SEX – Male predilection
Mostly solitary
Bilateral and multiple cysts – usually found in association with some syndromes – Example – CLEIDOCRANIAL DYSPLASIA, MAROTEAUX–LAMY SYNDROME
Dentigerous cysts may grow to a large size before diagnosed. Most discovered on radiographs when these are taken because a tooth has failed to erupt/ a missing tooth/ teeth are tilted/malalignment
Occasionally painful, particularly if infected
Potentially capable of becoming an aggressive lesion causing:-
Expansion of bone with subsequent facial asymmetry
Extreme displacement of teeth
Severe root resorption of adjacent teeth
Pain
Cystic involvement of an unerupted mandibular third molar may result in ‘hollowing-out’ of the entire ramus with displacement of the third molar to such an extent that it sometimes comes to lie compressed against the inferior border of the mandible
RADIOGRAPHIC FEATURES
Radiolucent area associated in some fashion with an unerupted tooth crown
Usually a smooth, unilocular lesion
Occasionally multilocular
Well-defined sclerotic margins unless they become infected
Distinction between a small dentigerous cyst and an enlarged dental follicle or follicular space is quite arbitrary, especially since they are histologically identical
Normal follicular space is 3–4 mm
Dentigerous cyst – Follicular space more than 5 mm. Only when the size of the radiolucency is grossly pathologic, distinction be made with assurance
Dentigerous cyst (white arrows) surrounding right impacted mandibular third molar
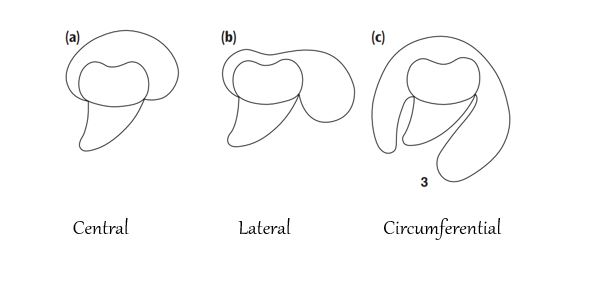
THREE RADIOLOGICAL VARIATIONS-
(a) Central variety – the crown is enveloped symmetrically. In these instances, pressure is applied to the crown of the tooth and may push it away from its direction of eruption. May push mandibular third at lower border of mandible or in the ascending ramus and a maxillary canine into maxillary sinus as far as the floor of the orbit
(b) Lateral type – radiographic appearance results from dilatation of the follicle on one aspect of the crown. Commonly seen when an impacted mandibular third molar is partially erupted so that its superior aspect is exposed
(c) Circumferential type – follicle expands in a manner in which the entire tooth appears to be enveloped by cyst
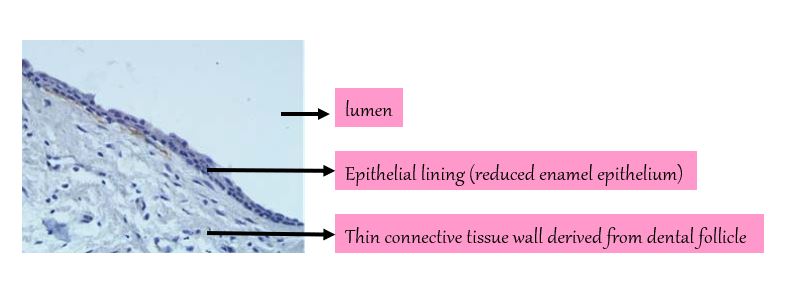
HISTOPATHOLOGIC FEATURES
Not characteristic microscopic features
Usually shows a:-
Thin fibrous cyst wall derived from dental follicle, consists of young fibroblasts widely separated by stroma and ground substance
Epithelial lining, which is in fact reduced enamel epithelium, consists of 2–4 cell layers of flat or cuboidal cells (a thin layer of stratified squamous epithelium lining the lumen)
Characteristically, the epithelial lining is not keratinized
Rete peg formation is generally absent except secondarily infected
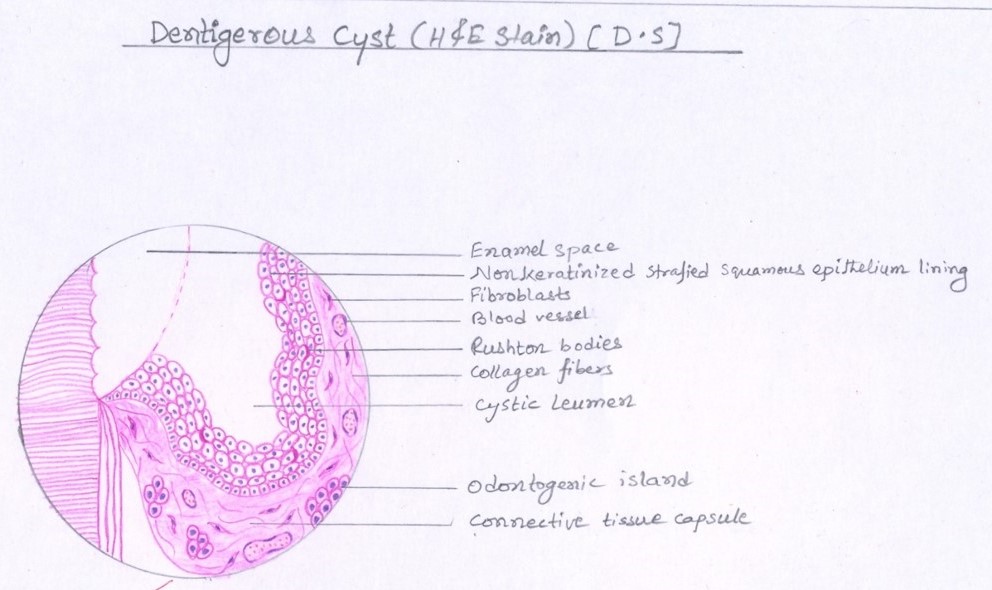
Connective tissue wall – of both normal dental follicles and dentigerous cysts is the presence of varying numbers of islands of odontogenic epithelium (sometimes sparse & inactive, while at other times in sufficient numbers)
Inflammatory cell infiltration of capsule common
Cysts which exhibit inflammation, may show presence of Rushton bodies within the lining epithelium. These are peculiar linear, often curved, hyaline bodies unknown origin (probably of hematogenous origin)
Content of cyst lumen – Usually thin, watery yellow fluid, occasionally blood tinged.
Intense inflammatory infiltrate in the adjacent capsule may lead to discontinuities in the epithelial
In some cysts, part of the epithelial lining may contain mucus-producing cells (result from metaplasia)
Dentigerous Cyst Oral Pathology Diagram
TREATMENT
Depends on size of lesion
Smaller cysts – Enucleation, Surgically removed in their entirety
Larger cysts – Marsupialization
Recurrence – Relatively uncommon
POTENTIAL COMPLICATIONS
AMELOBLASTOMA -From lining epithelium or from rests of odontogenic epithelium in the wall of the cyst
EPIDERMOID CARCINOMA
MUCOEPIDERMOID CARCINOMA – From the lining epithelium of the dentigerous cyst which contains mucus secreting cells, or at least cells with this potential ( common in dentigerous cyst with impacted mandibular third molars)



Thank you very much ma’am ❣️
Most welcome