
Hi Everyone, Sharing with you all what is Calcifying Epithelial Odontogenic Tumor. Study from this for your exams, score high and leave your comments below if these notes help you
OUTLINE
- OTHER NAMES
- DEFINITION
- ORIGIN
- CLINICAL FEATURES
- RADIOGRAPHIC FEATURES
- HISTOPATHOLOGIC FEATURES
- TREATMENT & PROGNOSIS
OTHER NAMES
- PINDBORG TUMOR
- Also called as CEOT (Calcifying Epithelial Odontogenic Tumor)
WHY CALLED A PINDBORG TUMOR????

First described in 1956 by the late Dr Jens J Pindborg, thus the name Pindborg Tumor

DEFINITION
The calcifying epithelial odontogenic tumor (CEOT) is a locally invasive epithelial odontogenic neoplasm, characterized by the presence of amyloid material that may become calcified.
- Benign
- Odontogenic neoplasm exclusively epithelial in origin
- Uncommon (CEOT accounts for approximately 1% of all odontogenic tumors )
ORIGIN
- The definite etiology of this neoplasm still remains enigmatic. Many authorities believe that it is derived either from:-

CLINICAL FEATURES
- AGE – Middle-age, patients between 20 and 60 years of age, with a mean around 40 years
- SEX – No gender predilection, equal frequency in both males & females

- SITE – More common in MANDIBLE

- Mandible :Maxilla = 2 : 1 i.e. about two thirds of cases found in mandible, most often in the posterior areas (prevalence in the molar region is three times that in the bicuspid region)
- Thus, most common site is MANDIBULAR MOLAR REGION
- Although Pindborg tumor shares clinical features with ameloblastoma as to site and age predilection, it is significantly less frequent in incidence
- Asymptomatic
- Painless swelling
- Slow growing expansile mass of the jaws
- 52% of reported cases associated with an unerupted or impacted tooth
- Most cases of CEOT are Intraosseous i.e. within bone
- Approximately 6% arise in extraosseous locations(i.e. outside bone). PERIPHERAL/EXTRAOSSEOUS lesions usually occur in the anterior gingiva. The extraosseous lesion is histologically identical with the intraosseous one
RADIGRAPHIC FEATURES
Considerable radiographic variation:-
- Diffuse or a well-circumscribed unilocular radiolucent area
- Or there may appear to be a combined pattern of radiolucency and radiopacity with many small, irregular bony trabeculae traversing the radiolucent area in many directions, producing a multilocular or honeycomb pattern.
- Scattered flecks of calcification throughout the radiolucency have given rise to the descriptive term of a ‘DRIVEN SNOW’ appearance.
- Some instances, the lesion is totally radiolucent and is in association with an impacted tooth, usually a mandibular third molar.
- Computed tomography and magnetic resonance imaging provide useful information in the diagnosis and treatment of CEOT
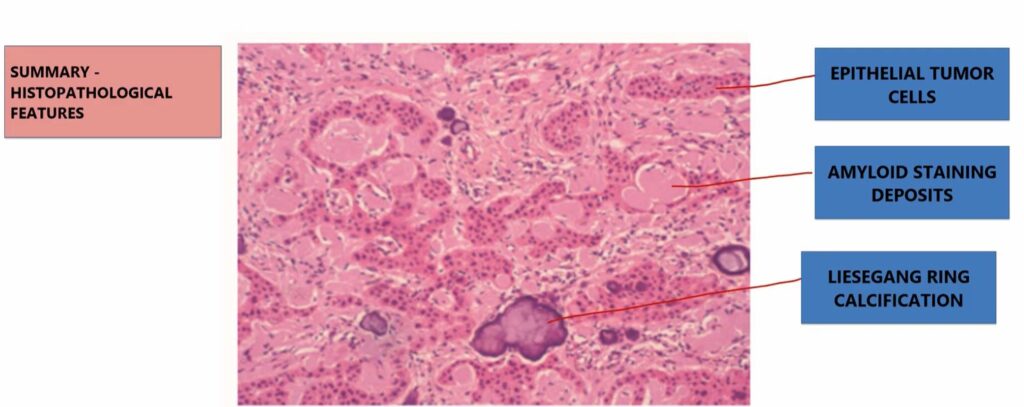
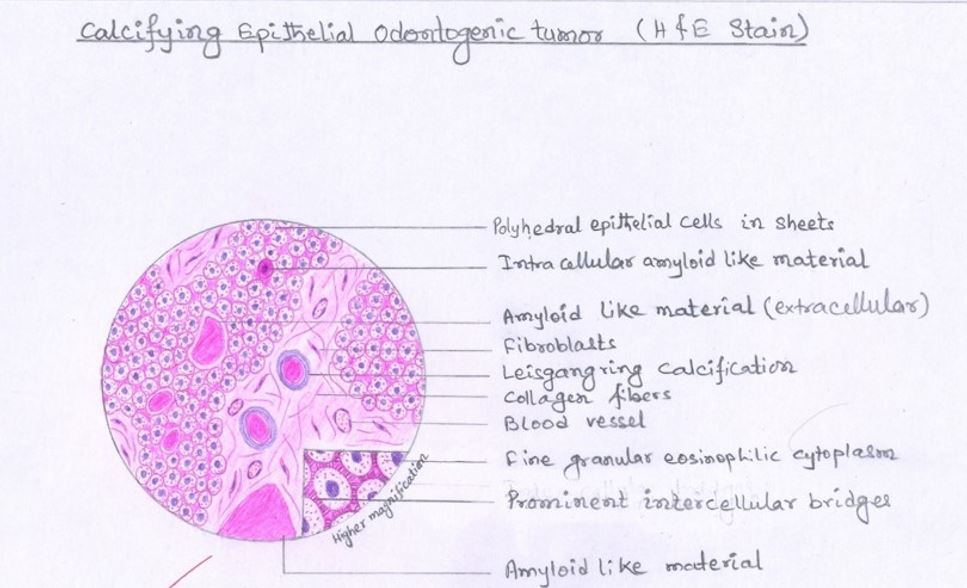
HISTOPATHOLOGIC FEATURES
- The tumor consists of a fibrous stroma with islands and sheets of polyhedral epithelial cells with:-
- abundant eosinophilic finely granular cytoplasm
- sharply defined cell borders
- well developed intercellular bridges
- The nuclei are:-
- frequently pleomorphic with giant nuclei and multinucleation being quite common
- mitotic figures rare
- Abundant, eosinophilic, homogeneous, hyaline material (AMYLOID) is present within or around the sheets of tumor cells. It is often calcified in the form of concentric rings (LIESEGANG RING CALCIFICATION)
 (liesegang ring means concentric rings) In CEOT calcification occurs in such rings
(liesegang ring means concentric rings) In CEOT calcification occurs in such rings
- One of the characteristic microscopic features of CEOT is the presence of a homogeneous, eosinophilic substance considered to be AMYLOID. This is so because it stains in a fashion similar to amyloid:-
- Positive staining with Congo red (shows apple green birefringence when subjected to polarized light)
- Stains metachromatically with crystal violet
- fluoresces under ultraviolet light with thioflavin T
- Some tumors are amyloid-rich, while others demonstrate epithelial-predominance.
- Clear-cell variant of CEOT – When Clear cells i.e. cells with clear cytoplasm within the epithelial nests are predominant
TREATMENT & PROGNOSIS
- CEOT is a locally invasive tumor
- An overall recurrence rate of about 14% has been noted
- Complete excision of the tumor with a border of normal bone should be curative, but recurrence follows incomplete excision
- Long-term follow-up is recommended
REFERENCES
- World Health Organization Classification of Tumors
- Shafer’s Textbook Of Oral Pathology
- Neville – Oral & Maxillofacial Pathology
- Image-Wikipedia & Wikimedia Commons