It’s a clinical term (based on the location of the lesion, clinical appearance, history given by patient etc.)
Mucocele on Lower Lip
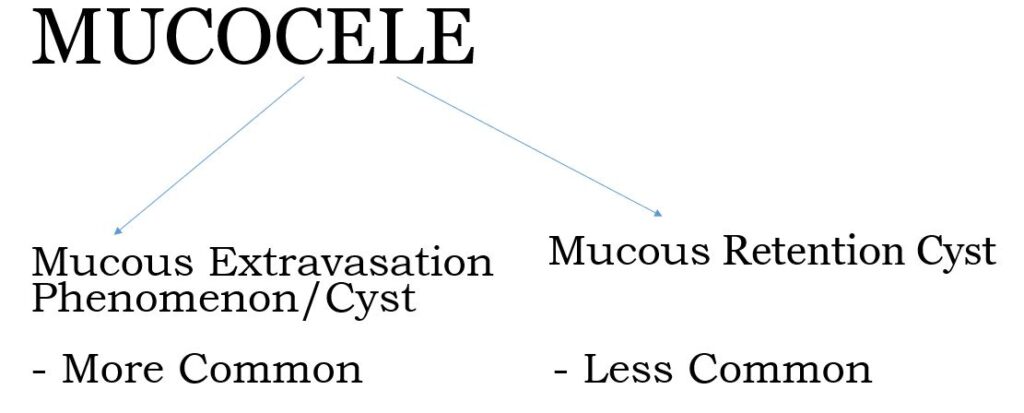
HISTO-PATHOLOGICALLY MUCOCELE IS OF TWO TYPES:-
MUCOUS EXTRAVASATION CYST
Lesions in which mucus has extravasated into connective tissue from a severed excretory duct
Mainly affect the minor salivary glands, particularly of the lip
Not a TRUE CYST ( no epithelial lining)
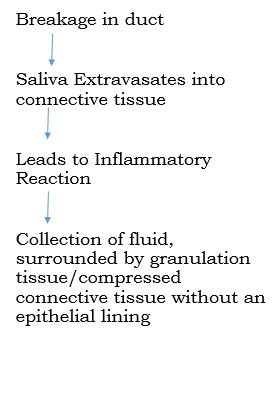
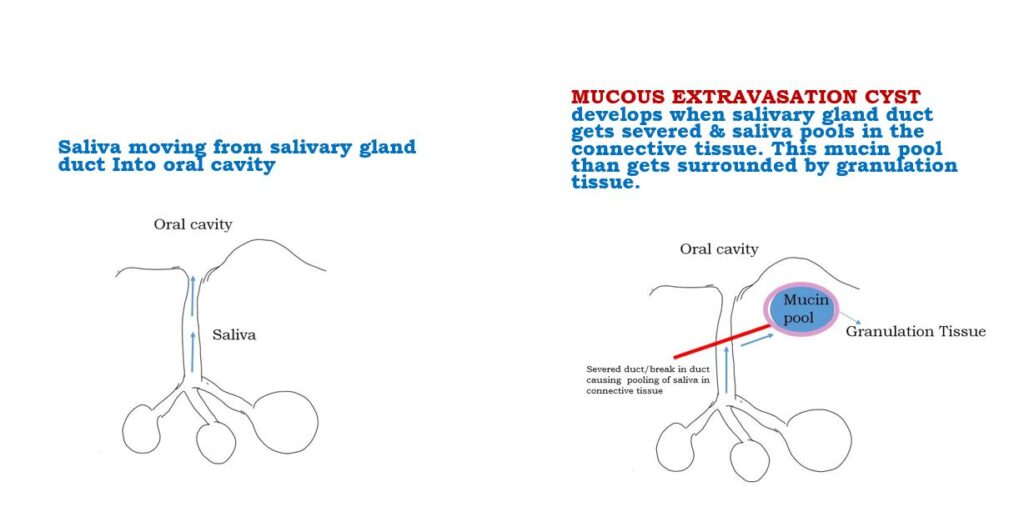
HOW IS A MUCOUS EXTRAVASATION CYST FORMED?
Normal Salivary Flow Phenomenon Vs How A Mucous Extravasation Cyst Is Formed
CLINICAL FEATURES
SITE:-
Most common site is Lower lip (as a result of injury or biting of mucosa)
Other sites-
buccal mucosa
floor of the mouth
ventral tongue
soft palate
retromolar area
upper lip is an uncommon site
AGE – Children & young adults
SEX PREDILECTION – Male = Female
Usually Superficial
SIZE – Rarely larger than 1 cm in diameter
APPEARANCE-Dome shaped swellings, fluctuant, translucent bluish due to thin wall
DURATION – Variable, Characteristic Finding – Alternate regression recurrence due to the cystic cavity getting rupture and re-accumulation of saliva. Post rupture, they create painful ulcerations which heal within days.
Sometimes SUPERFICIAL MUCOCELE (VARIANT) – Occur on soft palate, retromolar area and posterior buccal mucosa and they appear as 1-4 mm tense vesicles that burst leaving behind painful ulcers. This should not be confused with vesiculo-bullous lesions.
A large Mucocele in floor of mouth is called as Ranula
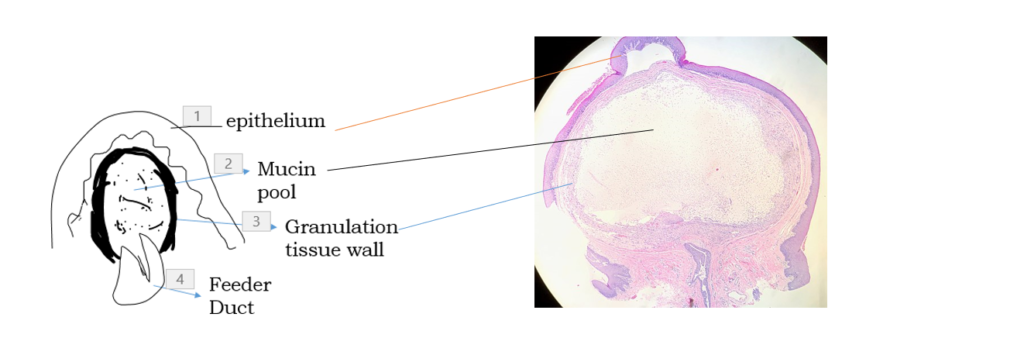
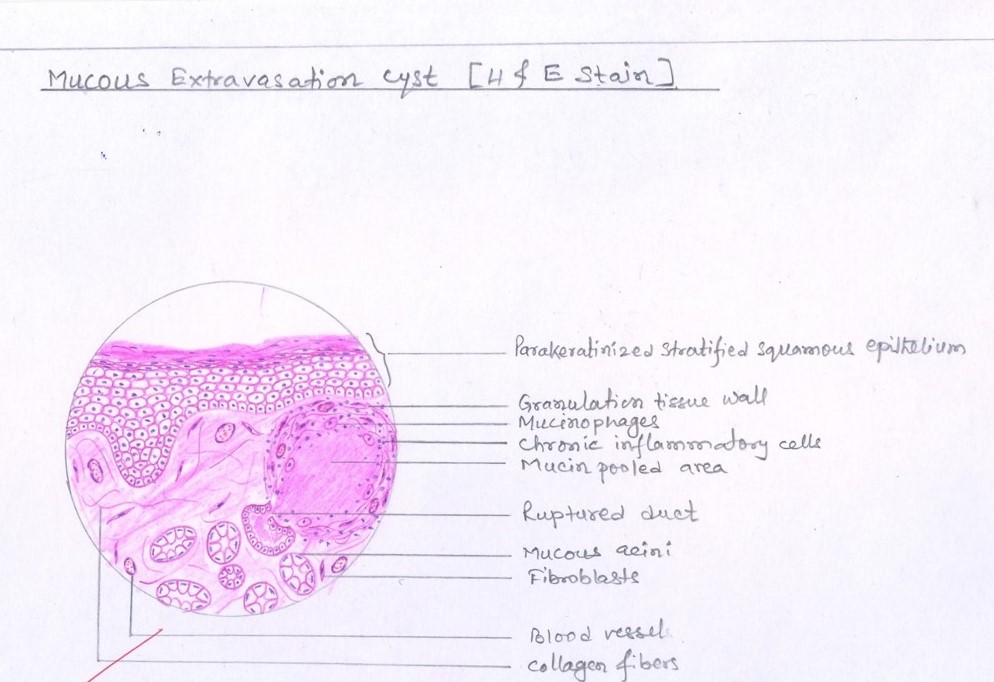
HISTOPATHOLOGIC FEATURES
Microscopically there is:-
Mucin Pool
Surrounded by Granulation Tissue Wall /compressed connective tissue wall in long standing lesions
No epithelial lining
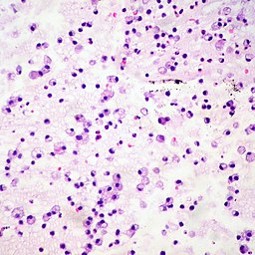
Prominent cells Mucinophages – Macrophages migrate into the mucin pool and by phagocytosing it develop foamy or vacuolated cytoplasm
Sometimes – Ruptured salivary duct feeding into the area (called as Feeder Duct)
Adjacent minor salivary glands often contain chronic inflammatory cell infiltrate & dilated ducts
MUCINOPHAGES
TREATMENT & PROGNOSIS
Short-lived lesions rupture and heal by themselves
Long Standing – Surgical Excision along with adjacent minor salivary gland tissue
Prognosis is excellent, although sometimes may recur, especially if feeding glands not removed
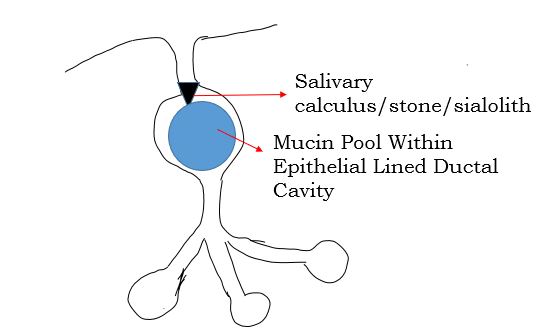
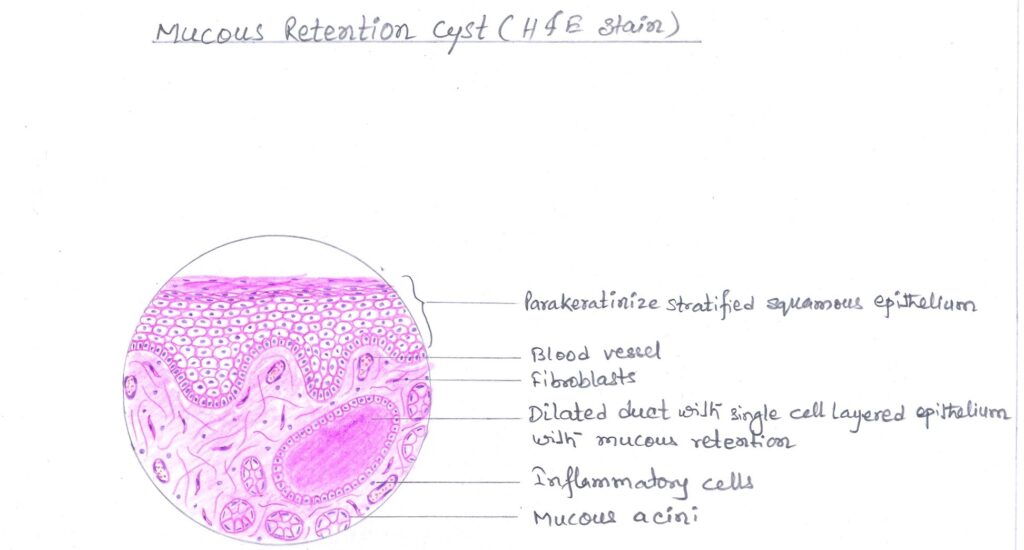
MUCOUS RETENTION CYST
Swelling due to obstruction of salivary gland excretory duct
Obstruction – salivary calculus/sialolith/salivary stone. Sometimes caused by periductal scarring or an impinging tumor
Accumulation of mucin within epithelial lined ductal cavity i.e. ductal dilatation secondary to obstruction
TRUE CYST – a retention cyst is lined by flattened/compressed ductal epithelium
Less common than mucous extravasation cyst
CLINICAL FEATURES
Clinically difficult to differentiate from mucous extravasation cyst
Affects adults
SITE
Major or minor salivary gland
Intraoral Cysts commonly involve minor salivary glands of floor of mouth, buccal mucosa, lips
Pain especially at meal time
HISTOPATHOLOGIC FEATURES
Epithelial lining is variable
May consist of cuboidal , columnar, or atrophic squamous epithelium surrounding thin or mucoid secretions in the lumen
The epithelium may undergo oncocytic metaplasia appearing as papillary folds into the cystic lumen
TREATMENT
Surgical Excision along with adjacent minor salivary gland tissue


best explanation mam
Thankyou