Outline
After reading this post you will learn the following about Mucoepidermoid Carcinoma:-
- Introduction
- Clinical Features
- Histopathologic Features
- Variants of Tumor
- Treatment & Prognosis
Introduction
- MUCOEPIDERMOID
CARCINOMA – As the name implies
-
Mucoepidermoid:- Composed of-
- Mucus-secreting Cells
- Epidermoid-type Cells
- Carcinoma means malignant epithelial tumor
- The mucus and epidermoid cells are in varying proportions
- Columnar and clear cells are also seen
- Often demonstrate prominent cystic growth
-
Mucoepidermoid:- Composed of-
- Most common malignant neoplasm in the major and minor salivary glands
- Accounts for 5% of all salivary gland tumors
- Most common site – Parotid Gland
- Intraorally, most common site is Palate
Clinical Features
- SEX – Slight female predilection
- AGE – Any age but occurs primarily in the third or fifth decades of life, with an average age of 47 years
- Most common
malignant salivary gland tumor of children
- Pathogenesis uncertain, although radiation exposure may be one risk factor
- Low Grade Tumor
- Slow growing
- Painless mass
- Rarely exceeds 5 cm in diameter
- Not completely encapsulated
- Often contains cyst filled with viscid mucoid material
- Intraoral Sites – Palate (most common), buccal mucosa, tongue & retromolar areas
- High Grade Tumor
- Rapidly growing swelling
- Pain is an early symptom
- Facial nerve paralysis frequent in parotid tumors
- Other Complaints – Trismus, difficulty in swallowing, drainage from ear, numbness of adjacent areas, ulceration (especially in tumors involving minor salivary glands)
- Not encapsulated, tends to infiltrate surrounding tissue, also many cases metastasize to regional lymph nodes
- Distant Metastasis Common – Lung, bone, brain & subcutaneous tissue
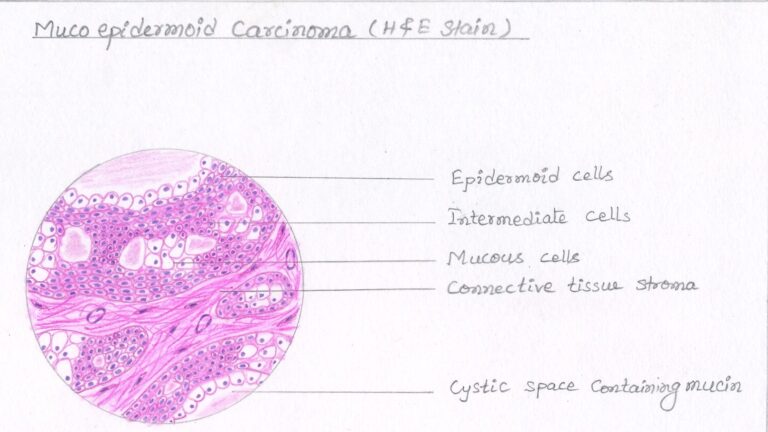
Histopathologic Features :-
- Mucoepidermoid
Carcinoma is composed of:
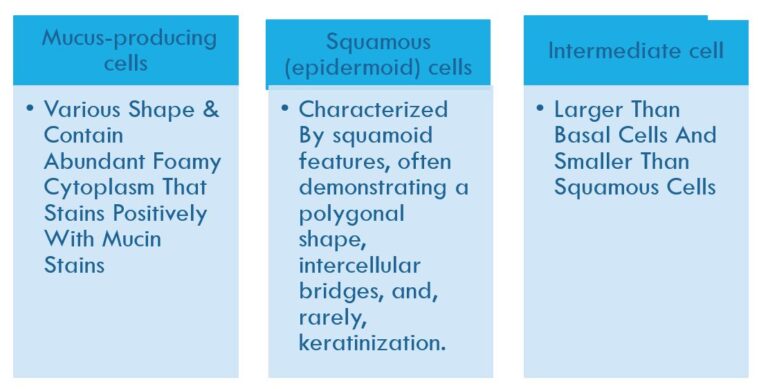
- Mucus-producing Cells
- Squamous (Epidermoid) Cells
- Intermediate Cells – More important in recognizing mucoepidermoid carcinoma. Highly prolific, basaloid cells. Thought to be a progenitor of both mucous and epidermoid cells.
Table Showing Features Of 3 Cell Types Seen In Mucoepidermoid Carcinoma:-
- Some tumors also show variable numbers of clear cells.
- Epidermoid, mucous & intermediate cells line cystic space or form solid masses or cords.
- Epidermoid & mucous cells may be arranged in glandular pattern.
- Cysts may rupture & release mucin. This mucin may pool in the connective tissue and evoke an inflammatory reaction.
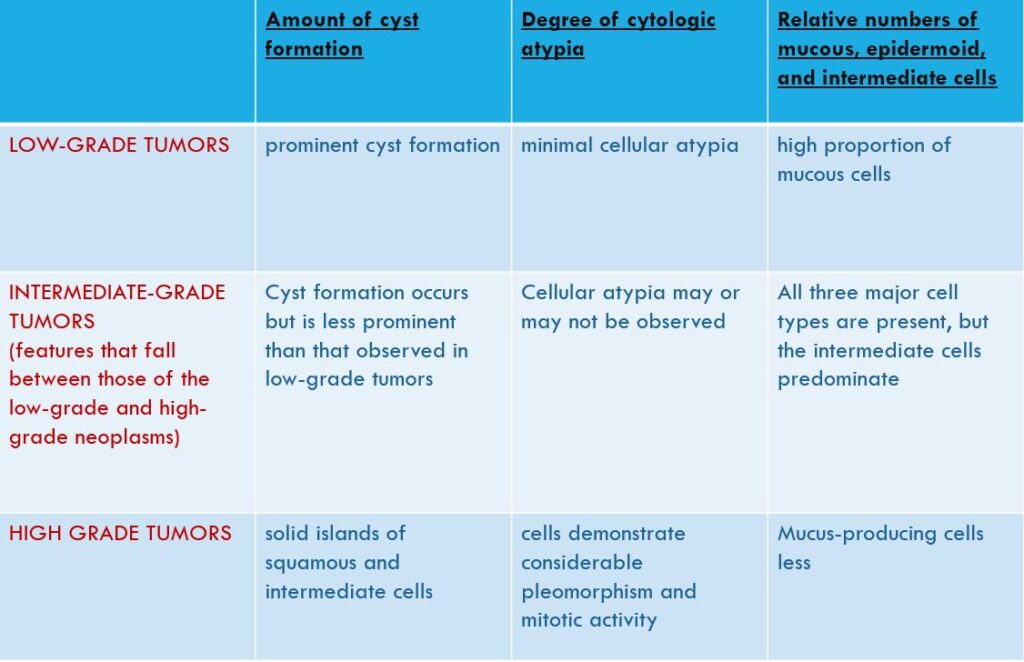
- Traditionally, mucoepidermoid carcinomas have been categorized into one of three histopathologic grades (LOW/INTERMEDIATE/HIGH) based on:
- Amount of cyst formation.
- Degree of cytologic atypia.
- Relative numbers of mucous, epidermoid, and intermediate cells.
TABLE SHOWING CRITERIA FOR CATEGORIZING MUCOEPIDERMOID CARCINOMA INTO 3 HISTOPATHOLOGIC GRADES – LOW, INTERMEDIATE & HIGH GRADE TUMOR
References :-
- Shafer’s Textbook Of Oral Pathology
- Shear – Cysts Of The Oral & Maxillofacial Regions
- Neville – Oral & Maxillofacial Pathology
- Image – Wikipedia & Wikimedia Commons
Variants Of Tumor
- Sclerosing Mucoepidermoid Carcinoma
- Intraosseous Mucoepidermoid Carcinoma
Treatment & Prognosis
- Low & intermediate-grade mucoepidermoid carcinomas of the parotid gland – Conservative excision with preservation of facial nerve, if possible, recommended
- Affected submandibular gland – Removed entirely
- If patient shows clinical evidence of cervical node metastasis/ T3 lesion – Radical neck dissection is performed
- Treatment for the minor glands – Primarily surgical
- For high grade tumors – Post-op Radiation & chemotherapy


